A 22 year old woman presented to our outpatient unit with the complaints of
Bilateral lower limb swelling since 1 month
Facial puffiness since 1 month
Shortness of breath since 1 month
Reduced urine output since 1 week
History of present illness :
1 month back, she first noticed bilateral lower limb swelling, pitting type upto her ankles which gradually extended to her thighs. Following this she also developed facial puffiness, significantly around her eyes which alarmed her and she paid a visit to our hospital and was started on conservative medications. However her symptoms did not subside. She started experiencing dyspnea on exertion which gradually progressed to an extent that she found it difficult to even walk for a short distance. She reported frothing of urine, however she had no hematuria. She complaints of reduced urine output since 1 week.
She did not have any history of chest pain, palpitations, giddiness, sweating.
She denied any history of fever, sore throat, rash, joint pains. No history of drug intake or antibiotic usage.
Past History:
12 years back, she was diagnosed with Type 1 Diabetes Mellitus on visiting a local hospital for fever and body pains. She has been receiving insulin injections since then.
In 2018, she was admitted in a local hospital for slurred speech which eventually became normal on normalising her blood sugar levels.
Her father reported that she had to be readmitted 2-3 times there after with the same complaints of slurred speech and hyperglycaemia. She was started on Injection Human Insulin Mixtard 18 units in the morning and 12 units at night.
6 months back, she was diagnosed with Hypertension on routine follow up and was started on Tab Telma 40mg once daily.
4 months back, she had an abortion at 7 weeks of gestation since the fetal heart beat couldn’t be assessed.
Personal History:
She currently lives with her parents who work as daily wage laborers. She has 2 elder sisters, who are married. She studied till 10th standard. She was married 1 year back to a farmer, however they haven’t been living together ever since her miscarriage.
Her mother reported decreased appetite since the last 2 months. She has only been consuming only milk, once to twice a day along with chapatti once in a day.

Problem Representation:
1. Generalized Anasarca
2. Dyspnea on exertion
3. Reduced urine output
4. Uncontrolled blood sugars
Provisional Diagnosis:
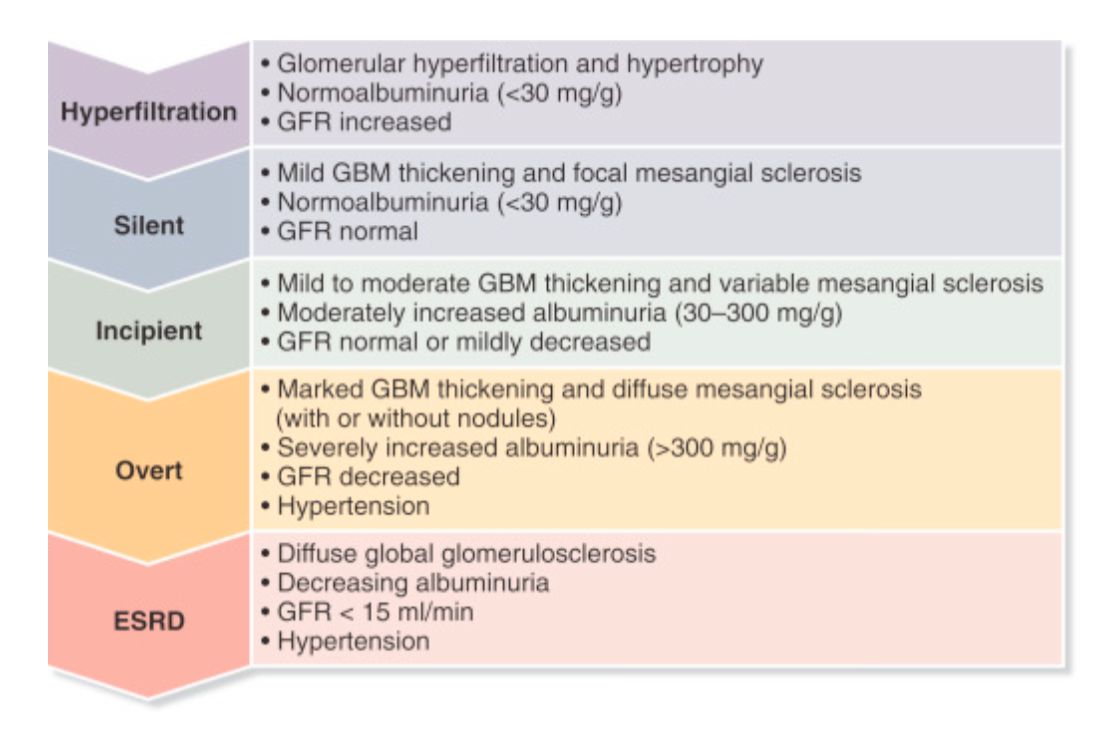
1. A 22 year old woman with significicant generalized anasarca, proteinruria and hypertension - Nephrotic Syndrome - ? Diabetic Nephropathy
2. Anemia secondary to ? chronic disease
3. Type 1 Diabetes Mellitus since 12 years
4. Hypertensive since 6 months
Clinical Examination:
General Examination:
Pulse Rate: 90 beats per minute, normal on volume, no radio-radial or radio-femoral delay
Blood Pressure: 150/70mmhg, right arm, supine posture
Respiratory Rate: 22 cycles per minute
Temperature: 98.6 F
Spo2: 98% on Room Air
GRBS: 260mg/dl
Height: 152.4 cm
Weight: 58 kgs
Body Mass Index: 23.2 kg/m
Waist circumference: 96 cms

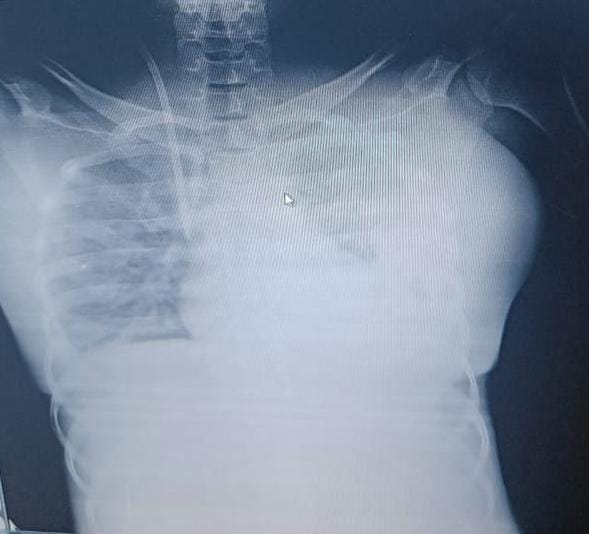
Images from previous admission:

.jpeg)
.jpeg)
Current admission pictures:
Head to toe:
Hair: Normal colour and texture, No areas of hair loss.

Eyes:
Pallor +
Periorbital edema +
Bilateral pterygium +
No cyanosis, icterus

.jpeg)




Bilateral lower limb edema, comparatively reduced due to Hemodialysis





.jpeg)



According to this the patients on intensive phase reduced risk of diabetic retinopathy, only 23 patients developed diabetic retinopathy and 91 patients on conventional therapy developed retinopathy.

.jpeg)
.jpeg)
In the two cohorts combined, intensive therapy reduced the occurrence of microalbuminuria by 39 percent, that of albuminuria by 54 percent, and that of clinical neuropathy by 60 percent.
No comments:
Post a Comment